
[Original article on ARCH+ here]
How sick is architecture?
Beatriz Colomina and Nikolaus Hirsch in conversation with Dennis Pohl about architecture, health, and biopolitics in the framework of the CIVA exhibition Sick Architecture in Brussels.
Dennis Pohl (DP): The title of your exhibition Sick Architecture is quite ambiguous. It can mean that architecture causes sickness or that architecture itself has become sick. How programmatic is this ambiguity?
Beatriz Colomina (BC): We like this ambiguity, of course. The exhibition is about expanding the range of our understanding what architecture is and what sickness is and about the intimate relationship between these two. Even if we try very much to deny it: sickness is a normal part of our life and architecture is pathological.
Nikolaus Hirsch (NH): The hypothesis we pursue is that architecture had from its very beginnings a problematic mission of hygiene. Architects – in their self-imagination – produce spaces of health.
BC: But it is a paradoxical relationship. As doctor Benjamin Ward Richardson put it when introducing Our Homes and How to Make them Healthy, a compendium of texts by doctors and architects for the 1884 International Health Exhibition in London: „Man, in constructing protection from exposure has constructed the conditions for disease.“ In other words, there is no disease without architecture and no architecture without disease. When moving indoors, we created the condition for diseases. The paradox is that architecture is always presenting itself as producing health, but it ultimately produces disease as well. For example, modern architecture advocated itself as being a kind of medical instrument to prevent tuberculosis with its white walls, terraces for the sun, the fresh air, etc. and yet this very architecture would eventually produce the so-called sick building syndrome, and put humans in contact with toxic materials.
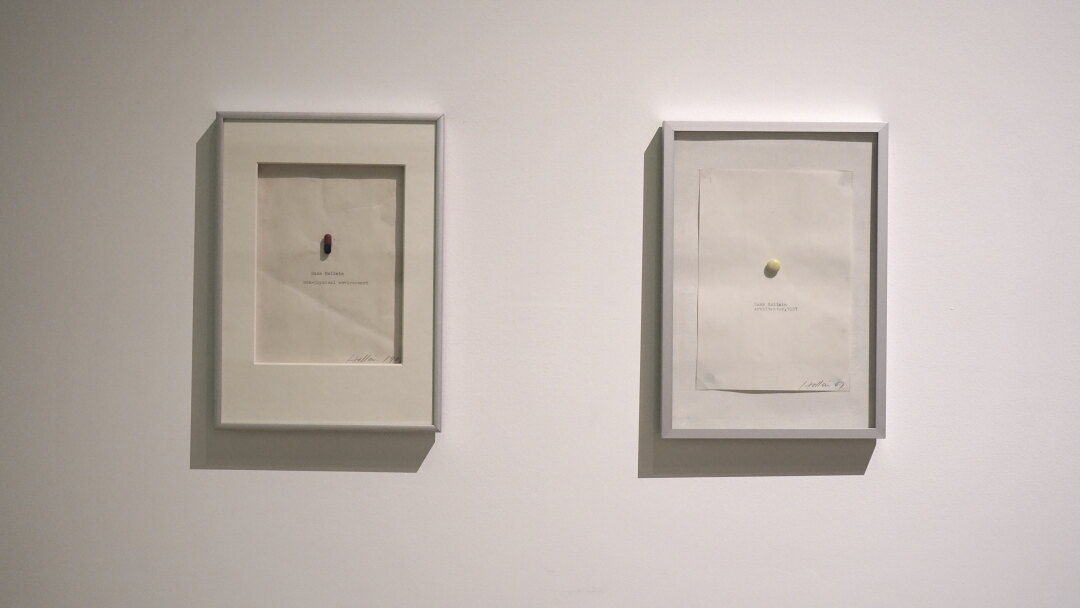
Hans Hollein: Non-physical environment, 1967, Private archive Hollein / Photo: Kristien Daem
DP: Consequently, the discourse of health and architecture is about more than just the question of hospital design. The perspective you open up is both transhistorical and transscalar, ranging from the territory to the pill.
NH: Looking backwards from today’s pandemic, you can see the production of sick architecture and its presumable healthy counterpart wherever you look.
BC: And transscalar literally means: from the scale of the pill which is a form of architecture, following Hans Hollein's „Alles ist Architektur“, that opens the exhibition to the little incubator that allows babies to survive despite frequent power cuts in sub-Saharan Africa and is like a little house, and even to a planetary scale, as shown by the contribution of Clemens Finkelstein, who researched how seismic networks measured the quietness of the Earth’s surface during COVID-19.1 In this sense, seismic activity informs us about the spread of a disease.
NH: One could even say the planet itself is sick. At a territorial scale, the work of Andrea Bagnato describes how the Italian coastline, once wetland paradise for malaria and mosquitoes, was dried out. Under Mussolini, land reclamation became a central project in the Fascist narrative, which was about hygiene, about health and against the so-called disease. Strategies to control malaria were clearly a political project going hand in hand with hygienic architecture and new forms of rural urbanization. It is a red thread in the exhibition: Many health policies and their architectural manifestations have been the perfect pretext to introduce discipline and control.
BC: This is also evident with the medicalization of borders. It became normal for us to travel with our QR codes, passenger locator forms, and COVID-19 certificates, but borders have always been medicalized. Think of Ellis Island, shown in the exhibition through the research of Guillermo Sánchez Arsuaga.2 Ellis Island’s architecture enabled an immigration process based on racialized and classed ideas of the healthy body. Or the Angel Island Immigration Station, that Jeremy Lee Wolin studied.3 It served to control Chinese immigrants using the excuse of health. Regardless of their actual health, racialized bodies are coded as unhealthy.
NH: These kind of border controls and border architecture have a strong link to today's situation with COVID-19 which is present in the exhibition, but we show their even longer territorial, political, and architectural history back to plague control, for example.
DP: One could say that architecture as a disciplinary apparatus always works on setting up the dividing threshold between notions of clean and dirty, interior and exterior, consumption and waste, white modernity and even colonial backwardness, or healthy and unhealthy. So architecture kind of performs on that line of the demarcation. This political dimension is probably most evident when at the scale of the territory architectural design is used as a device to separate.
BC: Yes, the political dimension is present in many forms. For instance, you may ask what has birth control in India to do with architecture? But then you see Shivani Shedde’s research on how housing policy, and even the designs of apartments, were intimately linked to family planning. Contraception wasn’t just done through pills. The housing unit itself served as a form of birth control.4 Even Buckminster Fuller advised Indira Gandhi on how computers, operational research, and general systems sciences could help India’s government to regulate the population.
NH: And they followed the classical model of the Western nuclear family: parents and two kids – which rarely existed in India.
BC: Either you follow that family model or you don't get a house.
DP: Architecture had always a very strong relation with diseases and epidemics. Maybe one kind of example that many are familiar with is cholera, and the way it was used to justify massive urban renewals and social reforms in the last centuries. But there are also more counter-intuitive examples like the work of Iván López Munuera, who studies the relation between architecture and HIV/AIDS.5 What other counterintuitive examples did you come across?
BC: Almost all of them are counterintuitive. It is really a research exhibition in that sense, from the individual contents of the participants to the exhibition design that overlaps the contributions in a way that invites the visitor to make new connections and ideas. The overall idea is that of a work in progress, a series of questions rather than answers. Our main goal was to expand the understanding of architecture, and of disease, and of their interdependence. There are many established architects, scholars and artists in the exhibition. Like Elizabeth Diller’s video on breathing during COVID-19 and Black Lives Matter, Philippe Rahm on COVID quarantine, Sammy Baloji on the Cordon Sanitaire in the Congo, or Fabiola López-Durán on the eugenic philosophy of modern architects, such as Le Corbusier and Lúcio Costa in Brazil.6 But there is also a whole army of young avant-garde scholars, such as Iván López Munuera on HIV/AIDS, Holly Bushman, who worked on the representation of menstruation and the control of women in Nazi Germany propaganda7, and Kara Plaxa on toxic masculinity8, and on and on.
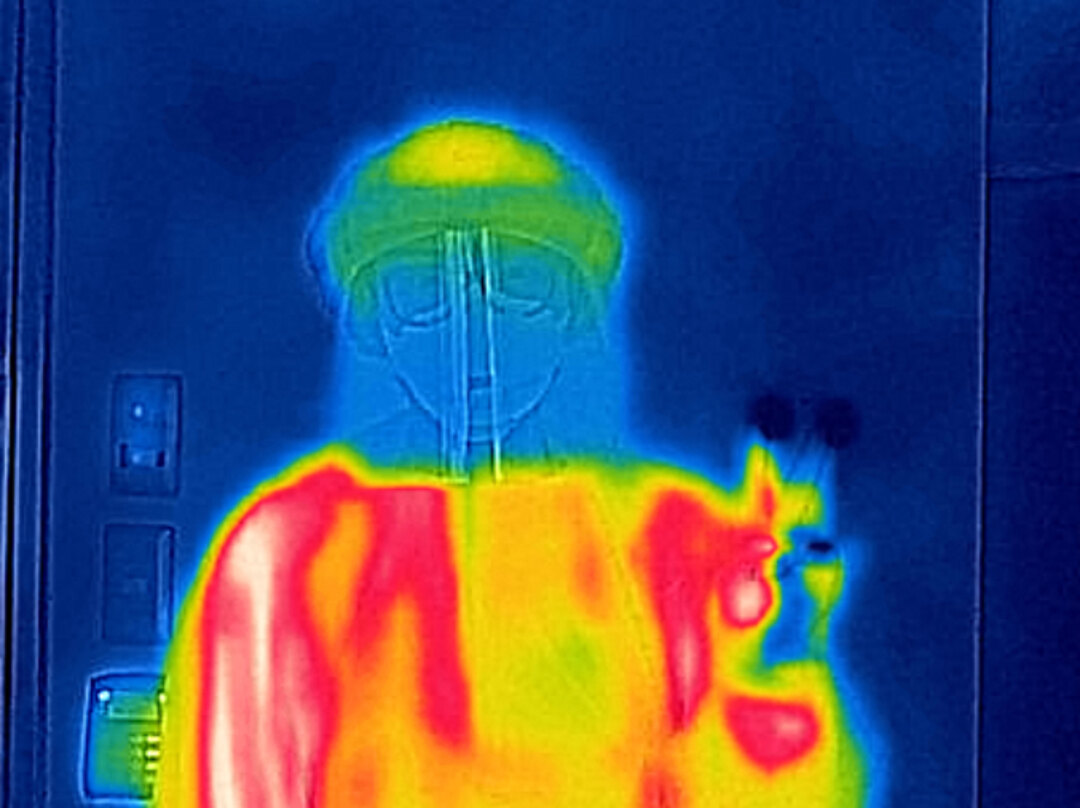
Philippe Rahm: The End of the Anthropocene, 2020, Photographs with thermal camera, Courtesy of Studio Philippe Rahm
DP: In Michel Foucault’s work architecture has a clear biopolitical framework to control the population, through prisons, hospitals, psychiatric clinics, etc. Did you come across works in your exhibition that go beyond this institutional framework?
NH: We have a number of examples which are more obviously speaking to this disciplinary architecture in a Foucauldian sense, like psychiatric hospitals. But we also considered the movements against the institution of the psychiatry itself with Susana Caló and Godofredo Peireira’s research La Borde and CERFI anti-psychiatry movements inspired by Felix Guattari9, Meredith TenHoor’s rediscovery of the forgotten architect Nicole Sonolet10, and contemporary repercussions in the Caritas psychiatry by De Vylder Vinck Tailleu.
BC: And there are also really unexpected themes like hunger. The work of Iason Stathatos considers hunger artists like „Jolly“ who spent days in glass cabins, constructed to turn starving into a spectacle.11 Even if hunger is not a sickness, it is a serious health problem and has its own architecture. There are many such unexpected cases such as autoimmune diseases, toxicity in general, eugenics, colonial medicine, alcohol abuse in indigenous communities, etc. These are all constructed diseases, diseases with a geopolitical history, technologies, designs and spaces.
DP: The exhibition entrance marks a symbolic situation. Hans Hollein’s Pill with the statement „Alles ist Architektur“ confronts the visitor in a Matrix-like choice: Take the blue pill to remain in contented ignorance, the red pill to learn a potentially life-changing truth. A pharmakon architecture in its multiple meanings. The Greek pharmakon can mean medicine, drug or poison. A substance with desirable positive effects, and side effects which are anyway coming with the same substance. In some sense one could speak of an architecture of pharmacology at the scale of the contraception pill or even the drug.
BC: It was an entire generation, not just Hans Hollein, who experimented with drugs, at a time when they were not yet forbidden. Journals such as Progressive Architecture in those years published articles about architecture on LSD. Richard Neutra did a house which functioned as a salon for LSD users, as Sylvia Lavin has shown.12 Neutra had previously presented his architecture as a form of prevention of tuberculosis with big windows and sleeping porches outside every bedroom for fresh air therapy. Neutra himself had suffered from Tuberculosis and was for a year in a sanatorium in Switzerland. His brother died of the disease. So it was also a personal trauma. But as soon as streptomycin – the first antibiotic effective against TB – was invented, Neutra declared his architecture to be good for mental health, the dominant disorder of the post-war years.
DP: So architecture functions like a pill or a medicine in itself. It can have some healthy effects, but it can also make people sick.

Sick Architecture, installation view of Alvar Alto’s designs for Paimio Sanatorium, Photo: Kristien Daem
BC: Yes, while for some architects, architecture is a kind of drug, for others, like Alvar Alto, architecture is a kind of medical equipment. He talks about architecture from a medical perspective. The whole question of rethinking what sickness is, can be found in Aalto’s statement when he says that architects always design for the vertical person, but here you have a client, the TB patient, that is constantly on the horizontal and therefore the architecture has to change. The vertical man goes back to the manuals of architecture that are always centered around the athletic healthy male figure, from Leonardo Da Vinci, to the Modulor of Le Corbusier. We are always designing for the able, white, exercised, body, but Aalto already said that architects should always „design for the person in the weakest position“. And the reality is that we spent significant parts of our lives in the weakest position, as a baby, when you are old, or you have a broken leg, or when you're pregnant or ill… So this myth that at the center of architecture there is this athletic, male, white, body, excludes most of the population. But in an architecture of disability we should design for those in the weakest position.
DP: In a way this project could be framed as a form of curatorial research, questioning the healthy body as a condition for modern architecture. How is this questioning of the normal reflected in the exhibition design?
BC: The exhibition itself is a form of research, as we were saying, it is an archive that exists in multiple media. It is shown here at CIVA in this beautiful installation by OFFICE Kersten Geers David Van Severen, but also in the series e-flux articles, podcasts and ongoing events.
The visitor, whether at CIVA or online, is basically not looking at an object on the wall or the screen, but somehow at the world itself, immersed in a kaleidoscopic array of symptoms of the entanglement of architecture and sickness. The contributions go back and forth in time, place and scale that forces the visitor to make their own connections. There is no particular sequence.
NH: So in that sense, there are no explicit chapters, no hierarchies, no didactics.
BC: No prescribed path or prescribed reading neither. It's more like an exploration of an almost overwhelming array of different juxtaposed thoughts.
NH: Crucial are the parameters of the exhibition design developed by OFFICE Kersten Geers David Van Severen. When usually doing an exhibition, you have the normative sight line at 1,50m, where you center things. But 1,50m is of course for standing person, not for people in wheelchairs, not for children.
BC: It is usually for men that are taller than most of the rest of us.
NH: What we developed is 20cm below this. So every video screen is centered much lower. This has an incredibly interesting effect on the space: The folded Plexiglas structure feels very low, hence the surrounding CIVA space much bigger. And it's very generous because this kind of folded Plexiglas structure is relatively low.
BC: In terms of content, there are several panels dealing with the question of architecture and disabilities. We have research by David Gissen, who has worked extensively with a team on the connection between architecture and the spectrum of capacities of human bodies.13 Then the research of Ignacio González Galán on Berkeley in the 60’s and the Center for Independent Living, where physical accessibility was introduced as a topic of architectural education. This came out of heated political debates, protests and strikes that were taking place on campus at the time, starting with the Free Speech movement in 1964. The ambition to give equal access to diversely abled bodies led some faculty and the students from the School of Architecture to collaborations in creating the conditions for an accessible campus. Policy changes that followed these events, eventually turned into the Americans with Disabilities Act in 1990.
NH: Disability architecture today is shown in a new, so far unpublished project by 51N4E in Brussels, which tries to „normalize“ disability. So today architects develop spatial strategies to weave together the everyday lives of different (dis)abitlies and try to renegotiate thresholds, stairs, etc., building on the history of the Center of Independent Living.
BC: I think these questions are sometimes also biographical. Architects get to reflect upon the fact that they themselves are part of an expanded spectrum of abilities or even suffering disability and learning from that disability. Alvar Aalto, for example, had been sick at the time of the commission of Paimio and claimed that having to stay in bed for such a long time, changed his understanding of architecture. As we said earlier, Neutra is another example. If you scratch a bit the surface, all of them either had tuberculosis or had very close friends and relatives who suffered from it. So you cannot think about modern architecture without thinking about TB. But for me, Aalto is a very special case, because he's effectively making sickness normal. Different degrees of sickness define the human condition. There’s no such a thing as the perfect healthy human body. That is such an anomaly, that exists – if at all – only for a short period of time.
DP: As you point out, it is very often related to biographical situations, which make designers reflect upon the relation of health and architecture. One could say that also COVID has written itself into our biographies with various degrees of tragedy. To what extend do you think architects are already able to reflect this today?
NH: When one mentions COVID-19 in the cultural sphere today, there is an obvious sense of oblivion. Everybody wanted to get back to normal – as if disease wasn’t normal. Our exhibition argues that the regime of Sick Architecture will not be over in a few months. Sickness has always been part of humankind. This is the thesis: Accept disease as the norm, and understand all these different, often contradictory aspects as part of the challenge for today's architects. That’s why we also show examples of today, like architecture from 51N4E with their Huis aan 't laar project as a laboratory for health care architecture, or De Vilder Vinck Architects with their Caritas psychiatric centre. I think what's interesting today is that many architects are seeing these topics as a source of innovation, and this is new – at least for the past 30 years.
BC: Yes, new and not new at the same time, because the generation of Le Corbusier, Neutra and Aalto was already concerned with that.
NH: It was a forgotten heritage, because after the heroic modernism and the anti-institutional experiments in the 70’s there was a kind of amnesia in our discipline. From the 80’s to the early 2000’s the least thing that architects were concerned about were hospitals and psychiatries. They were interested in museums to rise their cultural capital and hence architectural profile. I see these medical topics coming back to the architectural innovation, for instance with the striking example that we’re showing with the Maggie’s Centres.
BC: Maggies’s Centers is a project by Charles Jenck’s wife Maggie. After she was diagnosed with breast cancer, the first thing they realized was that the places where they had to spend time were horrible. Waiting in long corridors with no windows after you had just been diagnosed, for example, and they realized that the architecture was contributing to their feeling sick... Actually that kind of architecture is sick architecture. The Maggie's Cancer Caring Centres foundation was founded after her death. Maggie had already written about such a foundation in her diary, of which we have some documents on display. To start this program, many prominent architects like Zaha Hadid and Rem Koolhaas designed some of the earlier centers, giving the program significant visibility. These are not hospitals, they are places where people with cancer and their families and caregivers can go as a kind of sanctuary for rest and reflection. Gardens are a key part of the designs. An example that we have in the exhibition is designed by Benedetta Tagliabue and located on the campus of Sant Pau, that beautiful Art-Nouveau-hospital in Barcelona.
DP: Probably this exhibition hits the Zeitgeist of our time, as almost everyone has experienced during COVID that the question of pandemics or epidemics is a spatial concern. Everyone has experienced physically the effects of separation, enclosure, isolation, etc. Even thinking about architecture in your first e-flux event, that took place in the fall of 2020. It started in the middle of pandemics, resulting out of a seminar that you, Beatriz, taught at Princeton University.
BC: That's how we came to the idea of the exhibition. I was teaching on architecture and pandemics way before COVID. Many dissertation topics came out of that class. For example, the dissertation of Iván López Munuera on AIDS and architecture or Victoria Bugge Øye on Coop Himmelb(l)au’s experiments in collaboration with a local hospital in Vienna.14 All of this was at least two years before COVID-19. I was teaching a class about the normal and the pathological, which I continued in the fall of 2019 with another seminar on architecture and illnesses focusing on things like the cholera epidemics. When COVID happened in the middle of all of this, students asked me: „How did you know?“ Of course, I didn't know, even if we have been warned for a long time. So there was all this research work, and since students were very discouraged from not being able to go to class in person anymore, or to travel for research, the idea came up talking with Nikolaus and Nick Axel of doing the first e-flux series on Sick Architecture. The students became very keen and happy about it, as suddenly there was a goal. So the first e-flux series was the result of the pandemic.
NH: Including other high-profile voices.
BC: Yes, of course, we invited Elisabeth Povinelli with her work on the virus as a figure and an infrastructure.15 Mark Wigley wrote an article about chronic whiteness.16 More recently, we invited Fabiola López-Durán on eugenics and Modern architecture, Brooke Holmes on eugenics in Ancient Greece17, David Gissen on architecture and disabilities18, and Emily Apter with her contemporary analysis of COVID denialism19, among others.
NH: To weave all these different voices into an exhibition I think has been one of the driving forces for us. It was really important to have this very diverse, transdisciplinary group of participants. Researchers such as Meredith TenHoor, but also practicing architects, or artists like Vivian Caccuri on colonization through the lens of the mosquito and Sammy Baloji on the Cordon Sanitaire in the Congo.
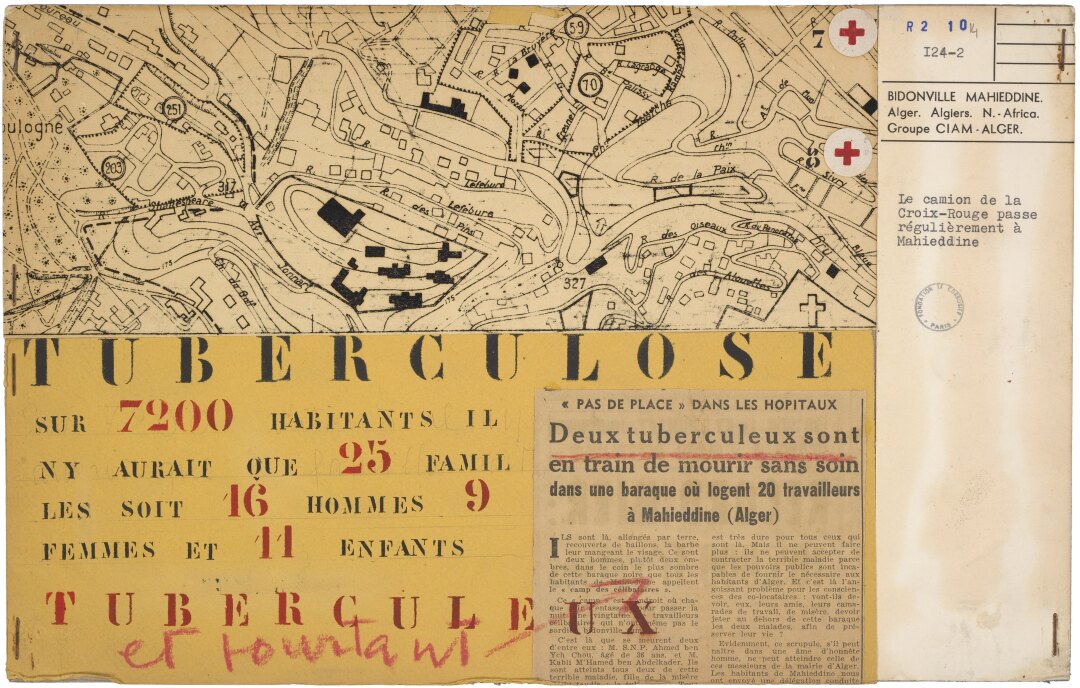
CIAM Algiers team, presentation panel on tuberculosis in Bidonville Mahieddinne, for the 9th CIAM congress in Aix-en-Provence, 1953, Fondation Le Corbusier
DP: About tuberculosis and modernism you wrote extensively in your book X-ray Architecture20. So after this exhibition, and after COVID, if there could be another chapter that you could still add to the book, what would that be?
BC: I would say, this chapter is written by the exhibition, and it is written in the best form that I could favor, which is collective. I have been doing this kind of collaborative work for a while now and the research work results in an exhibition, in a book, an event, etc. To open up the questions of X-ray Architecture was the starting point of this research, but it was at the same time a way to open up the question away from my own interests and expand the range of exploration that allows unexpected things to happen. Like, for example, AIDS and architecture, I guess one could have said before that AIDS has nothing to do with architecture, because it is not obvious, but Iván has showed us that it is deeply architectural. Likewise, it is not obvious that birth control or menstruation has something to do with architecture but Shivani and Holly have opened our eyes, just to refer again to the few examples we have touched on in this conversation. To allow such counter-intuitive suggestions and somehow follow them through and see how they develop, is very satisfying for me. As it is to collaborate with Nikolaus and Nick on e-flux in the texts, and in the exhibition. It expands our view. In that sense I almost prefer to disappear and let other generations think about it. I have learned so much about the topic in this way.
DP: If according to you diagnosis architecture is sick, do we want or need to make it healthy again, or are we already curing it? Or is that at all desired?
NH: What would be crucial for me is to pass beyond these dichotomies, beyond normal versus pathological, or healthy versus sick. Traditionally these dichotomies are used by architects for obvious purposes: to get commissions, or to invent briefs for new commissions. That's quite clear when you look into the examples that Foucault used to illustrate disciplinary architecture, from the hospital to the psychiatry. These buildings typologies and their institutions resulted from an alliance between doctors, architects, politicians and others to discipline society. So I think one can learn to be very careful and attentive when people promise „cure“. This is where I think such an exhibition and research project can provide tools for criticality, and maybe emancipation. One can learn to question briefs and rhetorics or to talk literally about what architecture does. This is crucial for me in the Maggie's Centers for instance: a collaboration between clients, architects. It shows a way to be critical about the status quo without promising the ultimate solution or cure. When you have cancer, there might be no solution because the end is – in many cases – relatively obvious. But still you can invent and work on a program which actually brings something positive for the people without saying this is sick and this healthy, this is normal or this is not normal.
BC: You cannot separate architecture from bodies, from things, and from minds. And bodies are always divergent, and in that sense sickness is always normal.
DP: Sickness is always there. I think this is a good conclusion of the intrinsic relation between architecture and illnesses, and the way how architecture always aimed to institutionalize, to normalize, and to produce the healthy body by contrast to what is unhealthy. One could speak of the compartmental imperative in the architecture of biopolitics. While there were – and I think this is very fascinating in this exhibition – movements which were counter-institutional or tried to get out of building heteronormative conceptions of spaces, bodies, and brains at the same time, by introducing alternative relations in the apparatus of architecture and health. So I think this is something very fascinating the exhibition tries to combine, first of all, a transhistorical perspective, but also exposing how the institutional and the counter-institutional are weaving into each other.
The exhibition Sick Architecture is ongoing at the CIVA in Brussels until August 28, 2022. For more information and the event calendar see: here, Twitter and Instagram.
1 Clemens Finkelstein: „Planetary Disequilibrium“, in: e-flux Architecture (May 2022), www.e-flux.com/architecture/sick-architecture/453873/planetary-disequilibrium/
2 Guillermo Sánchez Arsuaga: „Ellis Island – Architecture at the Service of Biopower“, in: e-flux Architecture (November 2020), www.e-flux.com/architecture/sick-architecture/345271/ellis-island-architecture-at-the-service-of-biopower/
3 Jeremy Lee Wolin: „The Finest Immigration Station in the World“, in: e-flux Architecture (May 2022), www.e-flux.com/architecture/sick-architecture/453869/the-finest-immigration-station-in-the-world/
4 Shivani Shedde: „Housing the Poor for a Healthy Planet and Healthy Nation“, in: e-flux Architecture (November 2020), www.e-flux.com/architecture/sick-architecture/345269/housing-the-poor-for-a-healthy-planet-and-healthy-nation/
5 Iván López Munuera: „Lands of Contagion“, in: e-flux Architecture (November 2020), www.e-flux.com/architecture/sick-architecture/363717/lands-of-contagion/
6 Fabiola López-Durán: „Fantasies of Whiteness“, in: e-flux Architecture (April 2022), www.e-flux.com/architecture/sick-architecture/461057/fantasies-of-whiteness/
7 Holly Bushman: „Regel-ated Bodies“, in: e-flux Architecture (June 2022), www.e-flux.com/architecture/sick-architecture/455119/regel-ated-bodies/
8 Kara Plaxa: „Boys will be Boys“, in: e-flux Architecture (November 2020), www.e-flux.com/architecture/sick-architecture/361128/boys-will-be-boys/
9 Susana Caló and Godofredo Pereira: „CERFI – From the Hospital to the City“, in: London Journal of Critical Thought (LJCT), vol. 1, issue 2 (June 2017): 83-100
10 Meredith TenHoor: „Care Beyond Biopolitics“, in: e-flux Architecture (May 2022), www.e-flux.com/architecture/sick-architecture/469553/care-beyond-biopolitics/
11 Iason Stathatos: „Hunger Architecture“, in: e-flux Architecture (May 2022), www.e-flux.com/architecture/sick-architecture/453870/hunger-architecture/
12 Sylvia Lavin: Form Follows Libido_ Architecture and Richard Neutra in a Psychoanalytic Culture, Cambridge, MA 2005
13 David Gissen: The Architecture of Disability – Buildings, Cities, and Landscapes beyond Access Minneapolis 2022
14 Victoria Bugge Øye: „On Astroballoons and Personal Bubbles“, in: e-flux Architecture (April 2018), www.e-flux.com/architecture/positions/194841/on-astroballoons-and-personal-bubbles/
15 Elizabeth A. Povinelli: „The Virus: Figure and Infrastructure“, in: e-flux Architecture (November 2020), www.e-flux.com/architecture/sick-architecture/352870/the-virus-figure-and-infrastructure/
16 Mark Wigley,: „Chronic Whiteness“, in: e-flux Architecture (November 2020), www.e-flux.com/architecture/sick-architecture/360099/chronic-whiteness/
17 Brooke Holmes: „On the Nature of Plato’s Embodied City“, in: e-flux Architecture (May 2022), www.e-flux.com/architecture/sick-architecture/453872/on-the-nature-of-plato-s-embodied-city/
18 David Gissen: „Disabling Form“, in: e-flux Architecture (May 2022), www.e-flux.com/architecture/sick-architecture/461056/disabling-form/
19 Emily Apter: „Live Free or Die? Psychopolitical Infrastructures of Denialism“, in: e-flux Architecture (June 2022), www.e-flux.com/architecture/sick-architecture/471538/live-free-or-die-psychopolitical-infrastructures-of-denialism/
20 Beatriz Colomina: X-Ray Architecture, Zürich 2019
{kind=link}